
SHARE
Prenatal Diagnosis and Testing
When Both Parents Have OI
If two people with OI have a child, there is a 75 percent chance that the child will inherit one or both OI genes, as follows: There is a 25 percent chance the child will inherit only the mother’s OI gene (and the father’s unaffected gene), a 25 percent chance the child will inherit only the father’s OI gene (and the mother’s unaffected gene), and a 25 percent chance the child will inherit both parents’ OI genes. Because this situation has been uncommon, the outcome of a child inheriting two OI genes is hard to predict. It is likely (even if both parents have mild OI) that the child would have a severe, possibly lethal, form of the disorder.
Carrier Screening of Parents
Carrier screening is a genetic test that identifies if you carry a gene with a change, or variant, that can impact your child. When performed before conceiving, genetic carrier screening can provide actionable knowledge and the opportunity to pursue alternative reproductive options. Carrier screening during pregnancy can help couples decide on prenatal or infant diagnostic testing, and if necessary, help them prepare emotionally, medically, and financially for a baby with OI.
Who can be a carrier of a genetic condition?
Everyone can be a carrier of a genetic condition regardless of ethnicity, family background, or family history.
What are some examples of companies that perform carrier screening?
- Horizon is a carrier screening service which screens for one or more genetic conditions through a single test.
*Disclaimer: The following company is an example of a carrier screening service. The OIF is not endorsed or sponsored by Horizon.
Prenatal Prognostication
While prenatal diagnosis can identify the presence of OI, predicting the exact type or severity of the disorder before birth is extremely challenging. Currently, there are no standardized methods or guidelines to accurately determine the type or severity of OI in utero, making it difficult to provide precise prognostic information to families.
Prenatal Diagnosis
Testing is available to help families further understand what type of OI someone has, provide some insight into the natural history of the condition (i.e., what the family can expect), and assist in prenatal diagnosis for families who wish to exercise that option. One of these tests examines collagen proteins to look for the quantitative or qualitative collagen defects that lead to OI. A second test is done directly on DNA from a blood sample and looks for a genetic mutation that causes OI. Because of the relatively small 2 to 4 percent risk of recurrence of Type II OI in a family, often due to gonadal mosaicism (a condition where the mutation is present only in the parent’s sperm or egg cells, not affecting their other body cells), many genetic centers now recommend very early ultrasound studies to determine if a developing fetus has the disorder. Women with OI who become pregnant, or women who conceive a child with a man who has OI, may also want to explore prenatal diagnosis. Undergoing prenatal diagnosis does not obligate parents to elect pregnancy termination, and the information obtained may be useful in managing pregnancy and delivery.
Prenatal Testing

Non-invasive prenatal testing using maternal blood (PreSeek™):PreSeek™ screens for various clinically significant and life-altering genetic disorders that are not screened for with current noninvasive prenatal screening (NIPS/NIPT) technology. The disorders screened for by this test often occur in the absence of a family history of the condition; the screen, developed by the genomic experts at Baylor Genetics in conjunction with Baylor College of Medicine, assesses fetal DNA for pathogenic and likely pathogenic variants in 30 genes.
Many of the disorders screened for on PreSeek™ are not associated with abnormal prenatal ultrasound findings, especially in the first trimester, or may not be evident until the pregnancy is more advanced or the child is born.
Ultrasound is the least invasive procedure for prenatal diagnosis, and therefore carries the least risk. Using ultrasound, a doctor can examine the fetus’ skeleton for bowing (bending of the leg or arm bones), fractures, shortening, or other bone abnormalities that may indicate OI. These bone abnormalities can be seen as early as 14 to 16 weeks gestation in infants affected by more severe types of OI, like Type II and Type III. Though ultrasound has been used occasionally to diagnose milder forms of OI, mild OI is often not detected until late in the pregnancy, if at all. There are different levels of ultrasound, some of which are more useful than others for detecting OI in a fetus. Even when ultrasound is performed by a highly qualified ultrasonographer, it may be difficult to accurately pinpoint the type of OI before birth.
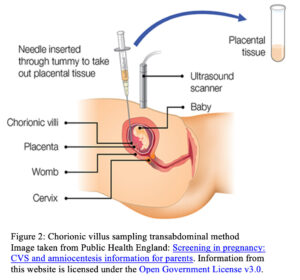
Chorionic villus sampling (CVS) examines placental cells, and, under some circumstances, can be used to detect abnormal collagen proteins or a genetic mutation that indicates that the fetus has OI. CVS can be performed at 10 to 14 weeks gestation. There is a 1 percent risk of miscarriage associated with CVS.
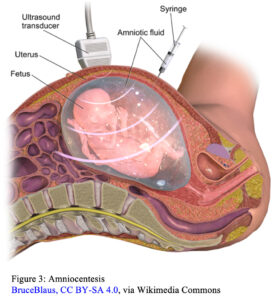
Amniocentesis examines fetal cells shed into the amniotic fluid. Because these cells carry all the genes that a fetus has inherited, amniocentesis can be used to look for a genetic mutation that causes OI. This technique is most useful when the mutation causing OI in a particular family has been identified through previous genetic testing of affected family members, including previous pregnancies involving a baby with OI. Amniocentesis is performed at 15 to 18 weeks gestation, and there is a 1 in 200 risk of miscarriage associated with the procedure.
Various circumstances affect the usefulness and accuracy of these tests. Not all types of tests are available in all geographic areas. When CVS or amniocentesis are used to attempt prenatal diagnosis of a fetus that has a parent with OI, it is helpful for the affected parent to have the results of his or her own collagen or DNA test available. Families are encouraged to discuss these techniques with their physician, as well as a geneticist and/or genetic counselor, to learn more about which techniques are appropriate for their situation.
Note: The information in this fact sheet is of a general nature. Families should seek counseling from a qualified physician or genetics clinic.